While you’re breastfeeding, the tissue in your breasts may appear dense on a mammogram, making it hard to read. So, it’s best to wait until after you stop breastfeeding to get a routine screening mammogram.
Discuss the best timing to get a mammogram with your health care provider if you’re due for screening.
If you find a lump or other change in your breast while you’re breastfeeding, see your health care provider.
Mammograms save lives by detecting breast cancer early enough to treat, and for most women, it’s important to have a mammogram every year beginning at age 40. For women who have a family history of breast cancer, annual mammogram screenings may start much earlier. One of the common questions we get from new moms is whether it’s safe to have a mammogram when breastfeeding.

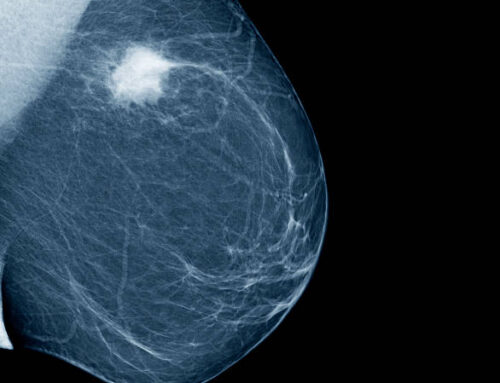
Mammogram
Mammography (also called mastography) is the process of using low-energy X-rays (usually around 30 kVp) to examine the human breast for diagnosis and screening. The goal of mammography is the early detection of breast cancer, typically through detection of characteristic masses or microcalcifications.
Where to get a mammogram
Mammograms can be done in:
- Radiology and imaging centers
- Mammography clinics
- Hospital radiology departments
- Mobile vans
- Some doctors’ offices
Can I get a mammogram while breastfeeding?
Since this is a question we are frequently asked, we thought that we’d share an excellent resource on this topic. This information is excerpted from a now defunct site ‘Best for Babes’ by Dr. Shannon Tierney, Breast Oncology Surgeon at the Swedish Cancer Institute in Seattle, Washington.
Although breast cancers in lactating women are extremely rare they are known to occur.1 Changes or abnormalities of any kind in your breast should be investigated with the same level of concern regardless of whether you are breastfeeding or not. Research shows that breastfeeding is associated with reduced mortality in women with breast cancer.2
If you need a mammogram while you are breastfeeding, it can usually be performed on your lactating breasts.However it is not necessarily recommended for high risk (BRCA) women under 303 : your healthcare professional will be able talk through your options with you.
Contrary to advice sometimes given it is possible to read a mammogram of a lactating breast (breasts that produce milk are called lactating breasts). Due to milk production, there is more dense tissue present in a lactating breast than in a non-lactating one: this may make it harder to read the results. The amount of tissue in your breast depends on the frequency that your baby is breastfeeding, depending on the age and stage your baby is at you may not be able to do adjust the frequency of feeds. To help reduce the amount of milk prior to a mammogram, you could bring your baby and breastfeed immediately prior to the procedure.
Ask for a radiologist who has experience reading mammograms of breastfeeding women.
X-rays do not affect human milk4, so you can safely resume nursing immediately after the mammogram.
If the lump you’ve discovered needs closer examination, you can feed immediately after fine-needle aspiration as well as after a biopsy or other surgery. It is important to let your doctor and/or surgeon know that you are breastfeeding so they can select appropriate medications for you.
If you have a biopsy or surgery you may need to adjust breastfeeding positions for a time to avoid putting pressure on the sore spot, or to express milk while you heal.

How does lactation affect normal breast screening methods
- Mammogram CAN be done in a breastfeeding woman. Ideally, it should be done with an experienced mammographer who knows the woman is breastfeeding, as the images will be more complex. She should empty her breasts as much as possible right before the mammogram, either by nursing or pumping.
- Ultrasound CAN be done in a breastfeeding woman. Same issues apply. Ultrasound, incidentally, can actually be somewhat useful therapeutically for breaking up a clogged duct.
- MRI CAN be done in a breastfeeding mother, though it is not recommended just for routine screening (as is done in high risk women) because the sensitivity is lowered. Gadolinium, the dye used for MRIs of the breast, barely gets into milk and is not absorbed by the baby’s gut, so it is safe – no need to pump and dump. Milk cytology can be done, but it’s often low-yield. It does have the advantage of being noninvasive, but needs a specialized pathologist and doesn’t usually rule out cancer.
How does lactation affect a breast biopsy and breast surgery?
- Needle biopsies (fine needle aspiration and core biopsy) CAN be done in a breastfeeding mother. The smallest needle that will get the diagnosis should be used, but the risk of milk fistula, which is chronic milk leakage, is very rare. There is no research on the incidence of milk fistulas with biopsies, but it’s rare enough that when it happens it gets written up as case reports! Incisions around the areola should avoid the lower outer border to keep from injuring the 4th intercostal nerve, and radial incisions (or an approach similar to what is done for C-sections, where the skin incision is made to be cosmetic and the inner dissection is done in a radial fashion) are recommended. The breast should be kept well drained with nursing or pumping before and after. Use of a local anesthetic like lidocaine is safe – no need to pump and dump.
- Surgery on the breast CAN be done in a breastfeeding mother. Milk fistula is still a risk, though that risk may not be reduced much by weaning as the breast could continue to make milk for months after weaning. The surgeon should be very careful with her technique – minimizing unnecessary damage to the milk ducts and avoiding the central breast if possible. Radial incisions and avoiding the 4th intercostal nerve (see above) are recommended. The breast should be kept well drained with nursing and pumping before and after. Most types of anesthesia will be out of the milk by the time the patient is awake and alert – at most, pump and dump once.
LUMP IN BREAST
Finding a lump in your breast is scary! Fortunately, most lumps in a lactating mother’s breasts are either milk-filled glands or an inflammation, such as a blocked duct or mastitis. If the lump is tender, it is probably mastitis. Check out this page for information on treating mastitis.
If the lump does not go away after a week of careful treatment for a blocked duct/ mastitis or if you are experiencing sudden flu-like symptoms or a high fever, or are at all concerned, contact your healthcare provider. If you notice red streaks on your breasts seek medical attention as they are a sign of infection that, left untreated, can develop into sepsis, a life threatening complication of an infection.
How does lactation affect normal breast screening methods
- Mammogram CAN be done in a breastfeeding woman. Ideally, it should be done with an experienced mammographer who knows the woman is breastfeeding, as the images will be more complex. She should empty her breasts as much as possible right before the mammogram, either by nursing or pumping.
- Ultrasound CAN be done in a breastfeeding woman. Same issues apply. Ultrasound, incidentally, can actually be somewhat useful therapeutically for breaking up a clogged duct.
- MRI CAN be done in a breastfeeding mother, though it is not recommended just for routine screening (as is done in high risk women) because the sensitivity is lowered. Gadolinium, the dye used for MRIs of the breast, barely gets into milk and is not absorbed by the baby’s gut, so it is safe – no need to pump and dump. Milk cytology can be done, but it’s often low-yield. It does have the advantage of being noninvasive, but needs a specialized pathologist and doesn’t usually rule out cancer.
What to expect
Preparing for a mammogram
Before the mammogram, you will undress from the waist up. So, it’s a good idea to wear a shirt you can remove easily.
Avoid using deodorants, antiperspirants, perfumes, powders or lotions on your breasts and underarm areas on the day of the exam. Ingredients in these products can show up on a mammogram and make it harder to read.
The mammogram procedure
During the exam, each breast is pressed between 2 plates and an X-ray image is made. Two views of each breast are taken, one with the X-ray beam aimed from top to bottom and the other from side to side.
Discomfort and anxiety
The pressure may be uncomfortable, but it only lasts a few seconds. If you have concerns, talk with your health care provider about taking acetaminophen (Tylenol) or ibuprofen (Advil, Motrin) before the exam.
Your health care provider can also discuss other ways to help ease discomfort (or anxiety) during a mammogram. Let your technologist know if you have any concerns before the exam, or if you feel any discomfort during the exam.
How long does a mammogram take?
Getting a screening mammogram takes about 15 minutes.

How does lactation affect a breast biopsy and breast surgery?
- Needle biopsies (fine needle aspiration and core biopsy) CAN be done in a breastfeeding mother. The smallest needle that will get the diagnosis should be used, but the risk of milk fistula, which is chronic milk leakage, is very rare. There is no research on the incidence of milk fistulas with biopsies, but it’s rare enough that when it happens it gets written up as case reports! Incisions around the areola should avoid the lower outer border to keep from injuring the 4th intercostal nerve, and radial incisions (or an approach similar to what is done for C-sections, where the skin incision is made to be cosmetic and the inner dissection is done in a radial fashion) are recommended. The breast should be kept well drained with nursing or pumping before and after. Use of a local anesthetic like lidocaine is safe – no need to pump and dump.
- Surgery on the breast CAN be done in a breastfeeding mother. Milk fistula is still a risk, though that risk may not be reduced much by weaning as the breast could continue to make milk for months after weaning. The surgeon should be very careful with her technique – minimizing unnecessary damage to the milk ducts and avoiding the central breast if possible. Radial incisions and avoiding the 4th intercostal nerve (see above) are recommended. The breast should be kept well drained with nursing and pumping before and after. Most types of anesthesia will be out of the milk by the time the patient is awake and alert – at most, pump and dump once.
When to expect results
Some centers give you the results of your mammogram at the time of your screening. With others, it may take up to 2 weeks to get your results.
If you don’t get your results within 2 weeks, contact your health care provider or the mammography center.
Don’t assume the results were normal because you didn’t get a report. Follow-up to get your results.
If you’re called back for more tests
If a finding is abnormal or the mammogram wasn’t clear enough for the results to be read, you will be called back for more tests.
Follow-up may include a diagnostic mammogram, breast ultrasound or breast MRI. In some cases, a biopsy may be needed.
It’s common to be called back for an abnormal finding on a mammogram. About 10-13 percent of women in the U.S. are called back after a mammogram for more tests. Try not to panic or worry.
Most abnormal findings are not breast cancer.
Sometimes, a mammogram shows something that looks like breast cancer when in fact, there’s no cancer in the breast. This is called a false positive result. The chance of having a false positive result after 10 yearly mammograms is about 50-60 percent.
Recall rates
The recall rate of a mammography center is the percent of women who are called back for more tests. Some centers may share their recall rate with you. This information may help you understand your chances of being called back.
Is it safe to have mammogram while breastfeeding?
Mammograms do not harm breastmilk; therefore, the procedure does not pose a risk to you or your infant
Should I pump and dump after mammogram?
The breast should be kept well drained with nursing or pumping before and after. Use of a local anesthetic like lidocaine is safe – no need to pump and dump. Surgery on the breast CAN be done in a breastfeeding mother.



{kind=link}
{kind=link}
{kind=link}
{kind=link}